Published Academic Articles
articles
Published Academic ArticlesBinocular Vision Correction for the Treatment of Vestibular Symptoms
A subtle vision misalignment, when identified with a thorough medical history and treated with aligning lenses, may reduce symptoms for some vestibular patients.
Binocular Vision Dysfunction and Vertical Heterophoria: A Brief History
Binocular vision dysfunction (BVD) encompasses a group of conditions where the two eyes have difficulty working together as a team, resulting in a vertical or horizontal (or both) misalignment between the line of sight of one eye with the other eye. When the amount of misalignment is large (strabismus or heterotropia) double vision or diplopia results. When the amount of misalignment is subtitle (heterophoria), single or fused imagery is maintained, but at the cost of overusing the vision alignment mechanisms, resulting in medical symptoms instead of diplopia.
As defined above, vertical heterophoria (VH) is a subset of BVD. Recently published research theorized that VH is occurring due to a lack of coordination between the two main vertical eye alignment mechanisms (the vision (or oculomotor) system and the balance (or vestibular) system) and that the initial problem is a faulty vertical alignment signal from the vestibular system1,2. If left unchecked, this would precipitate vertical double vision, which would be poorly tolerated. The oculomotor system appears to be identifying the misalignment and correcting it. These repetitive cycles of misalignment / realignment appear to lead to an overuse of the eye alignment muscles, which can result in the symptoms of VH. These include dizziness, headaches, anxiety, neck pain and difficulty with balance and coordination3,4,5,6,7,8,9,10,11.
The body may also try to correct VH (i.e.- to realign the images) by tilting the head, which can cause neck pain.
Causes
The two main causes of VH are brain injury (e.g. – TBI/concussion, stroke), and congenital causes. Both causes can occur at any age.
Why is VH not being diagnosed?
Although VH was first described in the 19th century7, the medical community has made little progress in identifying and treating this condition, most likely because the standard vision alignment tests are not sensitive enough to find these subtitle misalignments1,2,8,9,15,16,17,18,19,20.
The Diagnosis and Treatment of VH
The first step is to take a thorough medical history. VH has a very broad set of symptoms, many of which are not commonly appreciated by the medical community to be associated with a vision problem.
Symptoms
- Pain symptoms: headache, face ache/sinus pain, eye pain or pain with eye movements
- Head tilt symptoms: neck ache and upper back pain due to a head tilt
- Dizziness / Vestibular symptoms: dizziness, lightheadedness, off-balance feeling, motion sickness, nausea, poor depth perception, lack of coordination, unsteadiness or drifting to one side, disorientation
- Reading symptoms: difficulty with concentration, fatigue with reading, difficulty with reading comprehension, skipping lines, using a line guide (e.g. finger) to maintain one’s place, words running together, losing one’s place
- Routine visual symptoms: blurred vision, difficulty with close-up vision, difficulty with night vision, eye strain, sore eyes
- Binocular vision symptoms: double or overlapping vision, shadowed vision, light sensitivity, difficulty with glare or reflection, closing one eye while reading
- Psychological symptoms: feeling overwhelmed or anxious in a crowd, agoraphobia, feeling overwhelmed or anxious in large spaces (e.g. a mall)
To aid in obtaining a detailed history and to screen for those who might have VH, a validated questionnaire (Binocular Vision Dysfunction Questionnaire or BVDQ)21 can be used that includes questions from all of the major symptom groups and asks the patient to assess the frequency of their symptoms. A score of > 15 appears to be suggestive of VH.
Physical findings
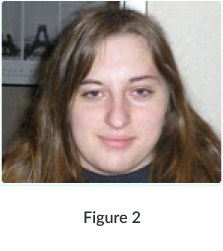
There are physical findings associated with VH, including the presence of a head tilt (Figure 1), a unilateral furrowed brow, an asymmetrical face (Figure 2), pulling to one side when walking, unsteady gait, and discomfort when observing a finger approaching your nose (convergence testing).

Establishing the diagnosis
Once a patient has been identified by their symptoms and/or physical findings as someone who may have VH, a complete ocular and vision exam is performed. Near sightedness, farsightedness and astigmatism must be identified and corrected prior to assessing the patient’s binocular vision status. Traditionally the next step in the assessment of VH involves the use of vertical alignment measurements such as vertical vergence, Von Graefe phoria testing at near and at far, cover test and red lens test. However, as previously mentioned, these tests are not sensitive enough to identify the subtle misalignments of VH1,2,13-20. To address this deficiency, an alternative technique for identifying the subtle vertical misalignment was developed. Named Prism Challenge, the technique consists of the incremental addition of small units of neutralizing vertical prism (usually 0.25D) to a trial frame containing the patient’s refractive prescription. The subtle vertical misalignment is identified (and the diagnosis of VH is established) when the patient, wearing the correct aligning (or prism) lenses for 10-20 minutes, experiences a marked reduction or even elimination of their VH symptoms.
Progressive Relaxation
In patients with VH, the eye alignment muscles are tense and over-worked and cannot relax quickly enough to allow the patient to wear the full amount of realigning prism immediately. Therefore, the first prescription contains less than the full amount of needed prism, and is worn for approximately 2-4 weeks. This allows the eye alignment muscles to experience Progressive Relaxation, after which the patient will be able to accept the full amount of prism needed (which is incorporated into their second set of lenses). Once treatment is completed (in about two visits), patients experience significant improvement, averaging an 80% reduction in symptoms.
Since VH is often not identified, many patients suffer for years without the proper diagnosis and treatment. Some patients may be told that their symptoms are due to migraines, atypical Meniere’s, psychogenic dizziness, anxiety and panic disorders, ADD/ADHD, as well as other conditions. Treatment for these conditions typically yields inadequate relief of symptoms.
Case Study
Sarah, a mechanical engineer, was injured in a car accident in which she suffered a traumatic brain injury (TBI). One year into her recovery she continued to experience a myriad of symptoms, including dizziness, headache, nausea, neck pain, eye strain, fatigue, and anxiety. She found it difficult to walk and drive and also had trouble focusing, reading, and writing. She received traditional treatment provided to patients with TBI but her symptoms did not improve.
By the time Sarah was referred for a specialized binocular vision evaluation (NeuroVisual evaluation) she was two years into her recovery and had been through speech therapy, occupational therapy, physical therapy, and vision therapy. Unfortunately, these treatments gave her only marginal relief from her symptoms. Sarah’s NeuroVisual evaluation revealed that she had a subtle vision misalignment (VH). She was prescribed aligning eyeglass lenses, and in a matter of minutes her symptoms were markedly reduced. Within one week her occupational therapist and neuropsychologist noted significant improvement. At the completion of treatment (8 weeks) her symptoms were reduced by 80% and she was able to live her life more fully, participating in many activities she wasn’t able to prior to wearing aligning lenses.
Research
Dr. Debby Feinberg and her research team have been researching VH since 1995, with the discovery that certain patients with dizziness actually had VH as the cause, and that treatment with aligning lenses immediately and markedly reduced symptoms22. It was then discovered that some TBI patients with persistent post-concussive symptoms had VH and responded to aligning lenses with a 70-80% reduction of symptoms23,24,25,26,27. It was also found that VH plays a role in certain patients with headache and anxiety28,29. A case series of 126 patients with VH was presented at the semiannual Barany Society meeting May, 2016 in Seoul, S. Korea.30
Summary
- Subtle vision misalignment can be congenital / spontaneous or precipitated by a brain injury / concussion, and has many non-visual symptoms including dizziness and other vestibular symptoms, headache, neck ache, anxiety, and difficulty reading.
- Head tilt during normal upright posture and difficulty with gait and balance are common physical signs.
- Current vision tests are not sensitive enough to find these subtle misalignments.
- People have suffered for years and have been incorrectly diagnosed with many other conditions, with the resulting treatment for those conditions providing only minimal relief.
- The diagnosis of VH is confirmed when the patient experiences immediate and marked reduction of symptoms with aligning eyeglass lenses.
- The average patient experiences an 80% reduction of symptoms by the end of treatment.
- The Binocular Vision Dysfunction Questionnaire (BVDQ) is a validated tool for identifying those who might have subtle vision misalignment.
The Authors
Dr. Debby Feinberg, owner of Vision Specialists of Michigan and Director of Clinical Care, Vision Specialists Institute, has been performing pioneering work with binocular vision dysfunction (BVD) and vertical heterophoria (VH). Her research has been presented locally, nationally and internationally, and published in peer reviewed journals. She is the author of a book about VH patients and their experiences with subtle vision misalignment and treatment with aligning lenses. She is Co-Director of the NeuroVisual Medicine Training Program, designed to train others to diagnose and treat subtle vision misalignment. She helped develop the Binocular Vision Dysfunction Questionnaire (BVDQ) that identifies patients that most likely have BVD and VH.

Dr. Mark Rosner is Director of Education and Research at Vision Specialists Institute, and a board certified Emergency Physician with more than 30 years of clinical experience. He has been actively involved in binocular vision dysfunction (BVD) and vertical heterophoria (VH) research since 2005, which has been presented locally, nationally and internationally, and published in peer reviewed journals. He helped develop the Binocular Vision Dysfunction Questionnaire (BVDQ) that identifies patients that most likely have BVD and VH. He is the co-author (with Dr. Feinberg) of “If The Walls of My Exam Room Could Talk”, a book about VH patients and their experiences with subtle vision misalignment and treatment with aligning lenses. He is Co-Director of the NeuroVisual Medicine Training Program, designed to train others to diagnose and treat subtle vision misalignment.

Doble JE, Feinberg DL, Rosner MS, Rosner AJ.
Identification of binocular vision dysfunction (vertical heterophoria) in traumatic brain injury patients and effects of individualized prismatic spectacle lenses in the treatment of postconcussive symptoms: A retrospective analysis.
Rosner MS, Feinberg DL, Doble JE, Rosner AJ.
Treatment of vertical heterophoria ameliorates persistent post-concussive symptoms: A retrospective analysis utilizing a multi-faceted assessment battery. Brain Injury
Borish IM.
History and Eye Strain.
Borish IM.
Analysis and Prescription.
Bixenman WW.
Vertical Prisms. Why Avoid Them? Surv of Ophthalmol.
Roy RR.
Symptomatology of Binocular Stress.
Duke-Elder S, Wybar K.
Anomalies of Binocular Fixation. Ocular Motility and Strabismus.
Staab JP, Ruckenstein MJ.
Expanding the Differential Diagnosis of Chronic Dizziness. Arch Otolaryngol Head Neck Surg.
Furman JM, Jacob RG.
Psychiatric Dizziness. Neurology.
Guerraz M, Yardley L, Bertholon P, et al.
Visual Vertigo: Symptom Assessment, Spatial Orientation and Postural Control. Brain.
Stevens, GT.
Functional Nervous Diseases. New York, NY: D. Appleton and Company
Karania R, Evans BJ.
The Mallet Fixation Disparity Test: influence of test instructions and relationship with Symptoms. Opthal. Physiol.
Wick BB.
Prescribing Vertical Prism: How Low Can you Go? Journal of Optometric Vision Development
Borish IM.
Clinical Refraction.
Duke-Elder S, Wybar K.
Anomalies of binocular fixation.
Gall R, Wick B.
The symptomatic patient with normal phorias at distance and near: What tests detect a binocular vision problem? Optometry
Gray LS.
The prescribing of prisms in clinical practice. Graefe’s Archive for Clinical and Experimental Ophthalmology
Schroeder TL, Rainey BB, Goss DA, Grosvenor TP.
Reliability of and comparisons among methods of measuring dissociated phoria. Optometry & Vision Science
Schow T, Teasdale TW, Rasmussen MA.
Validation of the Vertical Heterophoria Symptom Questionnaire (VHS-Q) In Patients with Balance Problems and Binocular Visual Dysfunction after Acquired Brain Injury. Soj Psychology.
Rosner AJ, Feinberg DL.
Vertical heterophoria: a common cause of dizziness and headache. Otolaryngology-Head and Neck Surgery.
Feinberg DL, Doble JE.
A Common and Treatable Cause of Post-Traumatic Headache and Dizziness: Vertical Heterophoria Syndrome.
Doble JE, Feinberg DL, Rosner MS, Rosner AJ.
Identification of binocular vision dysfunction (vertical heterophoria) in traumatic brain injury patients and effects of individualized prismatic spectacle lenses in the treatment of postconcussive symptoms: A retrospective analysis.
Rosner MS, Feinberg DL, Doble JE, Rosner AJ.
A Retrospective Analysis of Vertical Heterophoria Treatment and Amelioration of Post-concussive Disorder Symptoms Via a Multifaceted Assessment Battery.
Feinberg DL, Rosner MS, Doble JE.
An Unsuspected But Treatable Cause Of Persistent Post-Concussive Symptoms: Vertical Heterophoria.
Rosner MS, Feinberg DL, Doble JE, Rosner AJ.
Treatment of vertical heterophoria ameliorates persistent post-concussive symptoms: A retrospective analysis utilizing a multi-faceted assessment battery. Brain Injury
Rosner MS, Feinberg DL, Zasler ND.
Chronic Headache Amelioration with Prismatic Lens Treatment of Vertical Heterophoria. Headache.
Rosner MS, Warren R, Feinberg DL.
Prism vs. Prozac: A Novel Approach to the Amelioration of Anxiety with Prismatic-Lens Treatment of Vertical Heterophoria.
Rosner MS, Feinberg DL, Rosner AJ.
Chronic Dizziness, Headache and Anxiety Improved By Treatment of Vertical Heterophoria: A Retrospective Analysis. Oral presentation.
Published online: November 2, 2016, Vestibular Disorders Association (VEDA).
Authors: Debby L. Feinberg, Mark S. Rosner

Poster presentation at: The Anxiety Disorders of America Annual Meeting, Arlington, VA, April 2012

Poster presentation at: The American Headache Society 54th Annual Scientific Meeting, Los Angeles, CA, June 2012

Poster presentation at: The American Academy of Otolaryngology – Head and Neck Surgeons Annual Meeting, September 2012

Posted in: Otology and Neurotology, January 2020
Authors: Debby L. Feinberg, OD, Mark S. Rosner, MD, Arthur J. Rosner, MD

Published in:Future Science | 2022 | FSO813
Authors: Cherylea J Browne, Paul Fahey, Stella R Sheeba, Margie H Sharpe, Mark Rosner, Debby Feinberg & Viviana Mucci

Published in:PM&R | Volume 2, 244-253, April 2010
Authors: Jennifer E. Doble, MD, Debby L. Feinberg, OD, Mark S. Rosner, MD, Arthur J. Rosner, MD
Published in: Optometry & Visual Performance | Volume 8 | Issue 1 | 2020, March
Authors: Debby L. Feinberg, Mark S. Rosner, Arthur J. Rosner

Posted presentation at: The American Academy of Optometry Annual meeting, November 10, 2016
Authors: Debby L. Feinberg, Mark S. Rosner, Arthur J. Rosner

Posted online:February 1, 2020, Vestibular Disorders Association (VEDA).
Authors: Debby L. Feinberg, Mark S. Rosner

Poster presentation at: The 9th World Congress on Brain Injury, Edinburgh, Scotland March 2012

Poster presentation at: The Anxiety Disorders of America Annual Meeting, Arlington, VA, April 2012

Authors: Mark S. Rosner, Debby L. Feinberg, Jennifer E. Doble & Arthur J. Rosner
Published in: The journal Brain Injury, February 2016.

Authors: Debby L. Feinberg, Mark S. Rosner
Published online: November 2, 2016, Vestibular Disorders Association (VEDA).
Watch these videos of BVD patient experiences:
Daria's Binocular Vision Story
Robin's Traumatic Brain Injury
Veteran's Story of Binocular Vision Dysfunction and Triumph over TBI